Ticagrelor in Patients with Stable Coronary Disease and Diabetes
Steg PG, Bhatt DL, Simon T, Fox K, Mehta SR, Harrington RA, Held C, Andersson M, Himmelmann A, Ridderstrale W, Leonsson-Zachrisson M, Liu Y, Opolski G, Zateyshchikov D, Ge J, Nicolau JC, Corbalan R, Cornel JH, Widimsky P, Leiter LA, Committee TS, Investigators
2019 • N Engl J Med • [pdf]
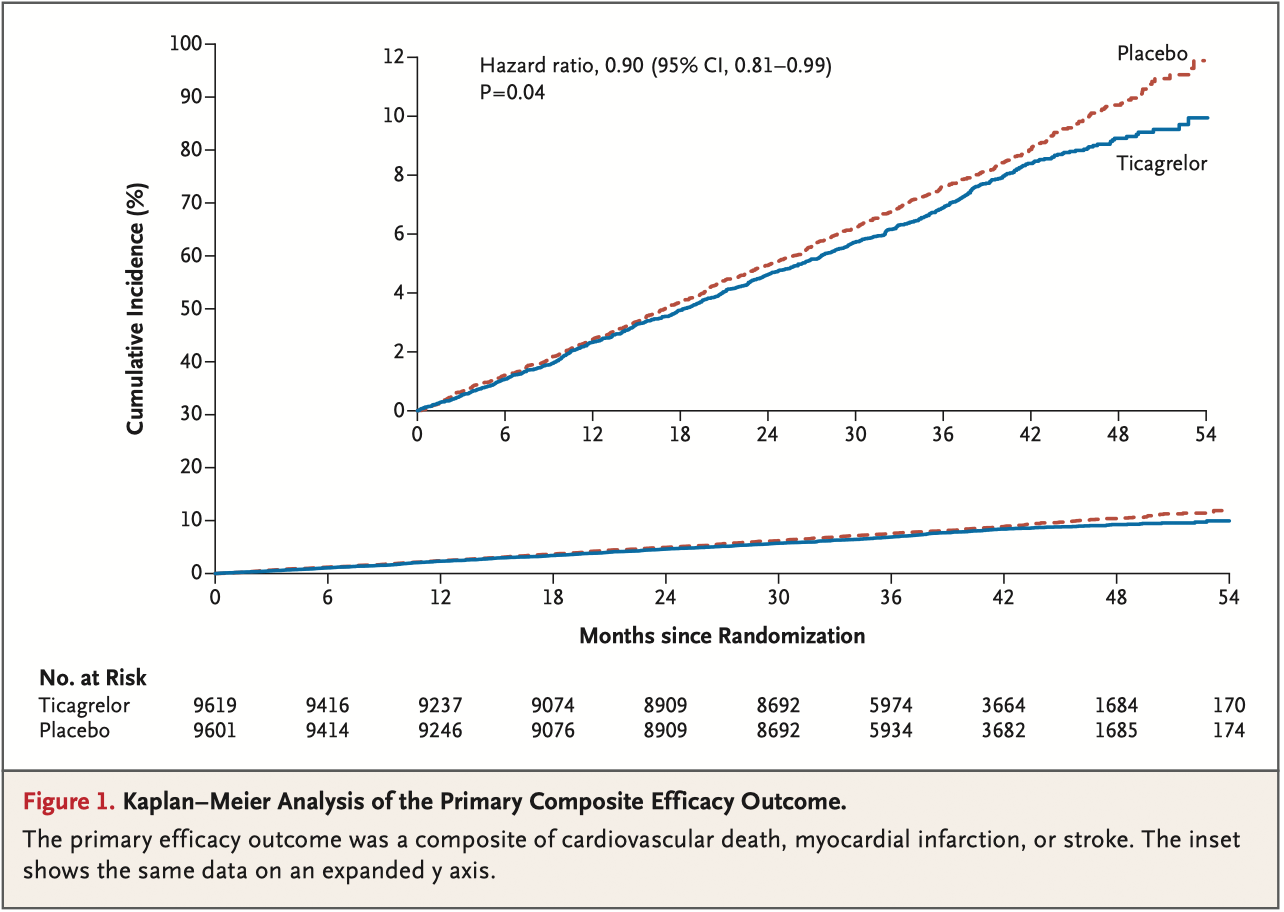
BACKGROUND: Patients with stable coronary artery disease and diabetes mellitus who have not had a myocardial infarction or stroke are at high risk for cardiovascular events. Whether adding ticagrelor to aspirin improves outcomes in this population is unclear. METHODS: In this randomized, double-blind trial, we assigned patients who were 50 years of age or older and who had stable coronary artery disease and type 2 diabetes mellitus to receive either ticagrelor plus aspirin or placebo plus aspirin. Patients with previous myocardial infarction or stroke were excluded. The primary efficacy outcome was a composite of cardiovascular death, myocardial infarction, or stroke. The primary safety outcome was major bleeding as defined by the Thrombolysis in Myocardial Infarction (TIMI) criteria. RESULTS: A total of 19,220 patients underwent randomization. The median follow-up was 39.9 months. Permanent treatment discontinuation was more frequent with ticagrelor than placebo (34.5% vs. 25.4%). The incidence of ischemic cardiovascular events (the primary efficacy outcome) was lower in the ticagrelor group than in the placebo group (7.7% vs. 8.5%; hazard ratio, 0.90; 95% confidence interval [CI], 0.81 to 0.99; P = 0.04), whereas the incidence of TIMI major bleeding was higher (2.2% vs. 1.0%; hazard ratio, 2.32; 95% CI, 1.82 to 2.94; P<0.001), as was the incidence of intracranial hemorrhage (0.7% vs. 0.5%; hazard ratio, 1.71; 95% CI, 1.18 to 2.48; P = 0.005). There was no significant difference in the incidence of fatal bleeding (0.2% vs. 0.1%; hazard ratio, 1.90; 95% CI, 0.87 to 4.15; P = 0.11). The incidence of an exploratory composite outcome of irreversible harm (death from any cause, myocardial infarction, stroke, fatal bleeding, or intracranial hemorrhage) was similar in the ticagrelor group and the placebo group (10.1% vs. 10.8%; hazard ratio, 0.93; 95% CI, 0.86 to 1.02). CONCLUSIONS: In patients with stable coronary artery disease and diabetes without a history of myocardial infarction or stroke, those who received ticagrelor plus aspirin had a lower incidence of ischemic cardiovascular events but a higher incidence of major bleeding than those who received placebo plus aspirin. (Funded by AstraZeneca; THEMIS ClinicalTrials.gov number, NCT01991795.).