External applicability of the COMPASS trial: an analysis of the reduction of atherothrombosis for continued health (REACH) registry
Darmon A, Bhatt DL, Elbez Y, Aboyans V, Anand S, Bosch J, Branch KR, Connolly SJ, Dyal L, Eikelboom JW, Fox KAA, Keltai K, Probstfield J, Yusuf S, Abtan J, Sorbets E, Eagle KA, Ducrocq G, Steg PG
2017 • Eur Heart J • [pdf]
Aims: The aims of the present study were to describe the proportion of patients eligible for the COMPASS trial within the Reduction of Atherothrombosis for Continued Health (REACH) registry, the reasons for ineligibility, and to put in perspective the characteristics and outcomes of trial-eligible patients from the REACH registry compared with those of patients enrolled in the reference aspirin arm of the COMPASS trial.
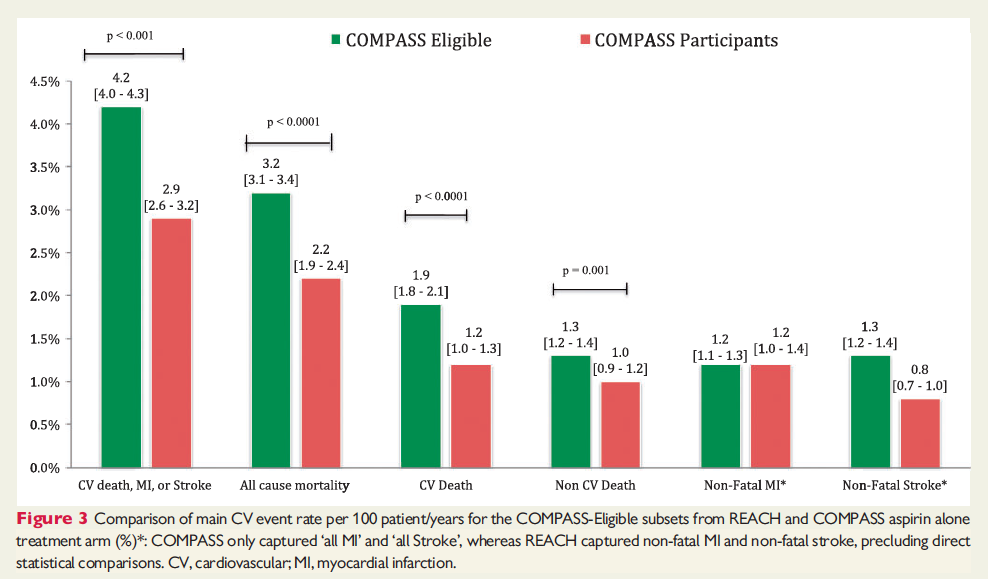
Methods and results: The COMPASS selection and exclusion criteria were applied to REACH patients with either coronary artery disease (CAD) or peripheral artery disease (PAD). We used the COMPASS primary composite outcome of cardiovascular (CV) death, myocardial infarction (MI), or stroke. In REACH, 31 873 patients had CAD or PAD and detailed information allowing evaluation of eligibility. Among these, 9518 (29.9%) patients had exclusion criteria and an additional 5480 patients (17.2%) did not fulfil the inclusion criteria and thus were not eligible. The ‘COMPASS-Eligible’ population therefore comprised 52.9% of the evaluable REACH patients (n = 16 875). The main reasons for exclusion were high-bleeding risk (51.8%), anticoagulant use (44.8%), requirement for dual antiplatelet therapy within 1 year of an ACS or PCI with stent, (25.9%), history of ischaemic stroke <1 year (12.4%), and severe renal failure (2.2%). Eligibility was highest among patients with PAD alone (68.4%). COMPASS-Eligible patients from REACH experienced higher annualized primary outcome event rates than patients actually enrolled in the reference aspirin arm of COMPASS (4.2% vs. 2.9% per year, P < 0.001).
Conclusion: COMPASS-Eligible patients represent a substantial fraction of stable CAD/PAD patients encountered in routine clinical practice in the large international REACH registry suggesting good external applicability. COMPASS-Eligible patients experienced a higher rate of the primary outcome compared with COMPASS participants in the aspirin alone treatment arm.